I'm not going to re-hash the paper in detail because that has been done elsewhere. However, I do want to make a few key points about the study and its interpretation. First, all groups had atherosclerosis to a similar degree, and it increased with advancing age. This suggests that atherosclerosis may be part of the human condition, and not a modern disease. Although it's interesting to have this confirmed in ancient mummies, we already knew this from cardiac autopsy data in a variety of non-industrial cultures (2, 3, 4, 5).
Read more �
Showing posts with label disease. Show all posts
Showing posts with label disease. Show all posts
Tuesday, March 12, 2013
Atherosclerosis in Ancient Mummies Revisited
Many of you are already aware of the recent study that examined atherosclerosis in 137 ancient mummies from four different cultures (1). Investigators used computed tomography (CT; a form of X-ray) to examine artery calcification in mummies from ancient Egypt, Peru, Puebloans, and arctic Unangan hunter-gatherers. Artery calcification is the accumulation of calcium in the vessel wall, and it is a marker of severe atherosclerosis. Where there is calcification, the artery wall is thickened and extensively damaged. Not surprisingly, this is a risk factor for heart attack. Pockets of calcification are typical as people age.
Thursday, January 3, 2013
Extreme Flu Activity in the US
A friend of mine came down with a nasty flu recently. I checked Google Flu Trends, and found that flu activity is currently at "intense" levels throughout the US. This is the highest flu activity Google Flu Trends has recorded in the last six years (image from Google Flu Trends 1/3/12).

Read more �

Wednesday, September 12, 2012
Nutrition Science Initiative (NuSI)
Some of you may have heard of an ambitious new nutrition research foundation called the Nutrition Science Initiative (NuSI). In this post, I'll explain what it is, why it matters, and how I feel about it-- from the perspective of an obesity researcher.
Monday, September 10, 2012
Calories and Carbohydrate: a Natural Experiment
In the lab, we work hard to design experiments that help us understand the natural world. But sometimes, nature sets up experiments for us, and all we have to do is collect the data. These are called "natural experiments", and they have led to profound insights in every field of science. For example, Alzheimer's disease is usually not considered a genetic disorder. However, researchers have identified rare cases where AD is inherited in a simple genetic manner. By identifying the genes involved, and what they do, we were able to increase our understanding of the molecular mechanisms of the disease.
The natural experiment I'll be discussing today began in 1989 with the onset of a major economic crisis in Cuba. This coincided with the loss of the Soviet Union as a trading partner, resulting in a massive economic collapse over the next six years, which gradually recovered by 2000.
Read more �
The natural experiment I'll be discussing today began in 1989 with the onset of a major economic crisis in Cuba. This coincided with the loss of the Soviet Union as a trading partner, resulting in a massive economic collapse over the next six years, which gradually recovered by 2000.
Read more �
Thursday, July 19, 2012
What Causes Type 2 Diabetes, and How Can it be Prevented?
In the comments of the last post, we've been discussing the relationship between body fatness and diabetes risk. I think this is really worth understanding, because type 2 diabetes is one of the few lifestyle disorders where 1) the basic causes are fairly well understood, and 2) we have effective diet/lifestyle prevention strategies that have been clearly supported by multiple controlled trials.
Read more �
Read more �
Thursday, July 12, 2012
Interview with Aitor Calero of Directo al Paladar
Aitor Calero writes for the popular Spanish cooking and nutrition blog, Directo al Paladar ("straight to the palate"). We did a written interview a while back, and he agreed to let me post the English version on my blog. The Spanish version is here and here.
Without further ado, here it is:
Read more �
Without further ado, here it is:
Read more �
Tuesday, April 17, 2012
Lessons From �tzi, the Tyrolean Ice Man. Part II
Otzi's Diet
Otzi's digestive tract contains the remains of three meals. They were composed of cooked grains (wheat bread and wheat grains), meat, roots, fruit and seeds (1, 2). The meat came from three different animals-- chamois, red deer and ibex. The "wheat" was actually not what we would think of as modern wheat, but an ancestral variety called einkorn.
Isotope analysis indicates that Otzi's habitual diet was primarily centered around plant foods, likely heavily dependent on grains but also incorporating a variety of other plants (3). He died in the spring with a belly full of einkorn wheat. Since wheat is harvested in the fall, this suggests that his culture stored grain and was dependent on it for most if not all of the year. However, he also clearly ate meat and used leather made from his prey. Researchers are still debating the quantity of meat in his diet, but it was probably secondary to grains and other plant foods. It isn't known whether or not he consumed dairy.
Read more �
Otzi's digestive tract contains the remains of three meals. They were composed of cooked grains (wheat bread and wheat grains), meat, roots, fruit and seeds (1, 2). The meat came from three different animals-- chamois, red deer and ibex. The "wheat" was actually not what we would think of as modern wheat, but an ancestral variety called einkorn.
Isotope analysis indicates that Otzi's habitual diet was primarily centered around plant foods, likely heavily dependent on grains but also incorporating a variety of other plants (3). He died in the spring with a belly full of einkorn wheat. Since wheat is harvested in the fall, this suggests that his culture stored grain and was dependent on it for most if not all of the year. However, he also clearly ate meat and used leather made from his prey. Researchers are still debating the quantity of meat in his diet, but it was probably secondary to grains and other plant foods. It isn't known whether or not he consumed dairy.
Read more �
Tuesday, April 10, 2012
Lessons From �tzi, the Tyrolean Ice Man. Part I

Otzi is Europe's oldest natural human mummy, and as such, he's an important window into the history of the human species in Europe. His genome has been sequenced, and it offers us clues about the genetic history of modern Europeans.
Otzi's Story
Read more �
Sunday, May 22, 2011
Fast Food, Weight Gain and Insulin Resistance
CarbSane just posted an interesting new study that fits in nicely with what we're discussing here. It's part of the US Coronary Artery Risk Development in Young Adults (CARDIA) study, which is a long-term observational study that is publishing many interesting findings. The new study is titled "Fast-food habits, weight gain, and insulin resistance (the CARDIA study): 15-year prospective analysis" (1). The results speak for themselves, loud and clear (I've edited some numbers out of the quote for clarity):
Read more �
Read more �
Saturday, April 16, 2011
Obesity and the Fluid-in, Fluid-out Therapy for Edema
I recently attended a lecture by Dr. Arya M. Sharma here at the University of Washington. Dr. Sharma is a Canadian clinician who specializes in the treatment of obesity. He gave the UW Science in Medicine lecture, which is a prestigious invited lecture.
He spent a little bit of time pointing out the fallacy behind conventional obesity treatment. He used the analogy of edema, which is an abnormal accumulation of fluid in the body.
Since we know that the amount of fluid contained in the body depends on the amount of fluid entering the body and the amount of fluid leaving the body, the treatment for edema is obvious: drink less, pee more.
Of course, this makes no sense. It doesn't address the underlying cause of edema and it will not help the patient. Yet we apply that exact same logic to fat loss. Since the amount of energy contained in the body (in the form of fat) depends on the amount entering and the amount leaving, the solution is easy: eat less, move more. Well, yes, if you can stick to that program it will cause fat loss. But that's equivalent to telling someone with edema to drink less water. It will cause a loss of fluid, but it won't correct the underlying problem that caused excessive fluid retention in the first place.
For example, if you have edema because your heart isn't pumping effectively (cardiac insufficiency), the heart is the problem that must be addressed. Any other treatment is purely symptomatic and is not a cure.
The same applies to obesity. If you don't correct the alteration in the system that causes an obese person to 'defend' his elevated fat mass against changes*, anything you do is symptomatic treatment and is unlikely to be very effective in the long term. My goal is to develop a method that goes beyond symptomatic treatment and allows the body to naturally return to a lower fat mass. I've been doing a lot of reading and I have a simple new idea that I feel confident in. It also neatly explains the results of a variety of weight loss diets. I've dropped a few hints here and there, but I'll be formally unveiling it in the next couple of months. Stay tuned.
* The body fat homeostasis system. The core element appears to be a negative feedback loop between body fat (via leptin, and insulin to a lesser degree) and the brain (primarily the hypothalamus, but other regions are involved). There are many other elements in the system, but that one seems to set the 'gain' on all the others and guides long-term fat mass homeostasis. The brain is the gatekeeper of both energy intake and energy expenditure, and unconscious processes strongly suggest appropriate levels for both factors according to the brain's perceived homeostatic needs. Those suggestions can be overridden consciously, but it requires a perpetual high degree of discipline, whereas someone who has been lean all her life doesn't require discipline to remain lean because her brain is suggesting behaviors that naturally defend leanness. I know what I'm saying here may seem controversial to some people reading this, because it's contrary to what they've read on the internet or in the popular press, but it's not particularly controversial in my field. In fact, you'll find most of this stuff in general neuroscience textbooks dating back more than 10 years (e.g., Eric Kandel and colleagues, Principles of Neuroscience).
He spent a little bit of time pointing out the fallacy behind conventional obesity treatment. He used the analogy of edema, which is an abnormal accumulation of fluid in the body.
Since we know that the amount of fluid contained in the body depends on the amount of fluid entering the body and the amount of fluid leaving the body, the treatment for edema is obvious: drink less, pee more.
Of course, this makes no sense. It doesn't address the underlying cause of edema and it will not help the patient. Yet we apply that exact same logic to fat loss. Since the amount of energy contained in the body (in the form of fat) depends on the amount entering and the amount leaving, the solution is easy: eat less, move more. Well, yes, if you can stick to that program it will cause fat loss. But that's equivalent to telling someone with edema to drink less water. It will cause a loss of fluid, but it won't correct the underlying problem that caused excessive fluid retention in the first place.
For example, if you have edema because your heart isn't pumping effectively (cardiac insufficiency), the heart is the problem that must be addressed. Any other treatment is purely symptomatic and is not a cure.
The same applies to obesity. If you don't correct the alteration in the system that causes an obese person to 'defend' his elevated fat mass against changes*, anything you do is symptomatic treatment and is unlikely to be very effective in the long term. My goal is to develop a method that goes beyond symptomatic treatment and allows the body to naturally return to a lower fat mass. I've been doing a lot of reading and I have a simple new idea that I feel confident in. It also neatly explains the results of a variety of weight loss diets. I've dropped a few hints here and there, but I'll be formally unveiling it in the next couple of months. Stay tuned.
* The body fat homeostasis system. The core element appears to be a negative feedback loop between body fat (via leptin, and insulin to a lesser degree) and the brain (primarily the hypothalamus, but other regions are involved). There are many other elements in the system, but that one seems to set the 'gain' on all the others and guides long-term fat mass homeostasis. The brain is the gatekeeper of both energy intake and energy expenditure, and unconscious processes strongly suggest appropriate levels for both factors according to the brain's perceived homeostatic needs. Those suggestions can be overridden consciously, but it requires a perpetual high degree of discipline, whereas someone who has been lean all her life doesn't require discipline to remain lean because her brain is suggesting behaviors that naturally defend leanness. I know what I'm saying here may seem controversial to some people reading this, because it's contrary to what they've read on the internet or in the popular press, but it's not particularly controversial in my field. In fact, you'll find most of this stuff in general neuroscience textbooks dating back more than 10 years (e.g., Eric Kandel and colleagues, Principles of Neuroscience).
Wednesday, March 23, 2011
Safflower Oil Study
A few people have sent me a new study claiming to demonstrate that half a tablespoon of safflower oil a day improves insulin sensitivity, increases HDL and decreases inflammation in diabetics (1). Let me explain why this study does not show what it claims.
It all comes down to a little thing called a control group, which is the basis for comparison that you use to determine if your intervention had an effect. This study didn't have one for the safflower group. What it had was two intervention groups, one given 6.4g conjugated linoleic acid (CLA; 50% c9t11 and 50% t10c12-CLA) per day, and one given 8g safflower oil. I have to guess that this study was originally designed to test the effects of the CLA, with the safflower oil group as the control group, and that the interpretation of the data changed after the results came in. Otherwise, I don't understand why they would conduct a study like this without a control group.
Anyway, they found that the safflower oil group did better than the CLA group over 16 weeks, showing a higher insulin sensitivity, higher HDL, lower HbA1c (a marker of average blood glucose levels) and lower CRP (a marker of inflammation). But they also found that the safflower group improved slightly compared to baseline, therefore they decided to attribute the difference to a beneficial effect of safflower oil. The problem is that without a control (placebo) group for comparison, there's no way to know if the improvement would have occurred regardless of treatment, due to the season changing, more regular check-ups at the doctor's office due to participating in a study, or countless other unforeseen factors. A control group is essential for the accurate interpretation of results, which is why drug studies always have placebo groups.
What we can say is that the safflower oil group fared better than the CLA group, because there was a difference between the two. However, what I think really happened is that the CLA supplement was harmful and the small dose of safflower oil had no effect. Why? Because the t10c12 isomer of CLA, which was half their pill, has already been shown by previous well-controlled studies to reduce insulin sensitivity, decrease HDL and increase inflammatory markers at a similar dose and for a similar duration (2, 3). The safflower oil group only looked good by comparison. We can add this study to the "research bloopers" file.
It's worth noting that naturally occurring CLA mixtures, similar to those found in pastured dairy and ruminant fat, have not been shown to cause metabolic problems such as those caused by isolated t10c12 CLA.
It all comes down to a little thing called a control group, which is the basis for comparison that you use to determine if your intervention had an effect. This study didn't have one for the safflower group. What it had was two intervention groups, one given 6.4g conjugated linoleic acid (CLA; 50% c9t11 and 50% t10c12-CLA) per day, and one given 8g safflower oil. I have to guess that this study was originally designed to test the effects of the CLA, with the safflower oil group as the control group, and that the interpretation of the data changed after the results came in. Otherwise, I don't understand why they would conduct a study like this without a control group.
Anyway, they found that the safflower oil group did better than the CLA group over 16 weeks, showing a higher insulin sensitivity, higher HDL, lower HbA1c (a marker of average blood glucose levels) and lower CRP (a marker of inflammation). But they also found that the safflower group improved slightly compared to baseline, therefore they decided to attribute the difference to a beneficial effect of safflower oil. The problem is that without a control (placebo) group for comparison, there's no way to know if the improvement would have occurred regardless of treatment, due to the season changing, more regular check-ups at the doctor's office due to participating in a study, or countless other unforeseen factors. A control group is essential for the accurate interpretation of results, which is why drug studies always have placebo groups.
What we can say is that the safflower oil group fared better than the CLA group, because there was a difference between the two. However, what I think really happened is that the CLA supplement was harmful and the small dose of safflower oil had no effect. Why? Because the t10c12 isomer of CLA, which was half their pill, has already been shown by previous well-controlled studies to reduce insulin sensitivity, decrease HDL and increase inflammatory markers at a similar dose and for a similar duration (2, 3). The safflower oil group only looked good by comparison. We can add this study to the "research bloopers" file.
It's worth noting that naturally occurring CLA mixtures, similar to those found in pastured dairy and ruminant fat, have not been shown to cause metabolic problems such as those caused by isolated t10c12 CLA.
Monday, March 14, 2011
Gluten-Free January Survey Data, Part II: Health Effects of a Gluten-Free Diet
GFJ participants chose between three diet styles: a simple gluten-free diet; a "paleo light" diet diet that eliminated sugar and industrial seed (vegetable) oils in addition to gluten; and a "paleo full monty" diet that only included categories of food that would have been available to our pre-agricultural ancestors. The data in this post represent the simple gluten-free diet group, and do not represent the other two, which I'll analyze separately.
To get the data I'll be presenting below, first I excluded participants who stated on the survey that they did not adhere to the diet. Next, I excluded participants who were gluten-free before January, because they would presumably not have experienced a change from continuing to avoid gluten. That left us with 53 participants.
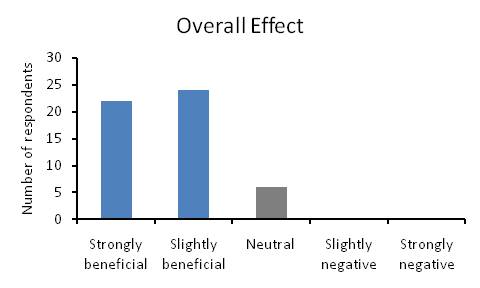
For each of these graphs, the vertical axis represents the number of participants in each category. They won't necessarily add up to 53, for several reasons. The most common reason is that for the questions asking about changes in health conditions, I didn't include responses from people who didn't have the condition in question at baseline because there was nothing to change.
Question #1: What is your overall opinion of the effect of gluten free January on you?
 Participants had a very positive experience with the gluten-free diet. Not one person reported a negative overall experience.
Participants had a very positive experience with the gluten-free diet. Not one person reported a negative overall experience.
Question #2: Did you note a weight change at the end of gluten free January?
 And here are the data for people who described themselves as overweight at baseline:
And here are the data for people who described themselves as overweight at baseline:
 Two-thirds of people who were overweight at baseline lost weight, and only one person out of 37 gained weight. That is striking. A number of people didn't weigh themselves, which is why the numbers only add up to 37.
Two-thirds of people who were overweight at baseline lost weight, and only one person out of 37 gained weight. That is striking. A number of people didn't weigh themselves, which is why the numbers only add up to 37.
Question #3: Before January 2011, did you have a problem with intestinal transit (frequent constipation or diarrhea)? If so, did your symptoms change during the month of January?

Responses are heavily weighted toward improvement, although there were a few instances where transit worsened. Transit problems are one of the most common manifestations of gluten sensitivity.
Question #4: Before January 2011, did you have frequent digestive discomfort (pain, bloating, etc.)? If so, did your symptoms change during the month of January?

Digestive discomfort was common, and the gluten-free diet improved it in nearly everyone who had it at baseline. I find this really impressive.
Question #5: Before January 2011, did you have acid reflux? If so, did your symptoms change during the month of January?
 Acid reflux responded well to a gluten-free diet.
Acid reflux responded well to a gluten-free diet.
Question #6: Before January 2011, did you have a problem with tiredness/lethargy? If so, did your symptoms change during the month of January?
 Lethargy was common and generally improved in people who avoided gluten. This doesn't surprise me at all. The recent controlled gluten study in irritable bowel syndrome patients found that lethargy was the most reliable consequence of eating gluten that they measured (1, 2). That has also been my personal experience.
Lethargy was common and generally improved in people who avoided gluten. This doesn't surprise me at all. The recent controlled gluten study in irritable bowel syndrome patients found that lethargy was the most reliable consequence of eating gluten that they measured (1, 2). That has also been my personal experience.
Question #7: Before January 2011, did you have a problem with anxiety? If so, did your symptoms change during the month of January?
 Anxiety tended to improve in most participants who started with it.
Anxiety tended to improve in most participants who started with it.
Question #8: Before January 2011, did you have a problem with an autoimmune or inflammatory condition? If so, did your symptoms change during the month of January?
 Autoimmune and inflammatory conditions tended to improve in the gluten-free group, although one person experienced a worsening of symptoms.
Autoimmune and inflammatory conditions tended to improve in the gluten-free group, although one person experienced a worsening of symptoms.
Question #9: If you ate gluten again or did a gluten challenge after gluten free January, what was the effect?
 Just under half of participants experienced moderate or significant negative symptoms when they re-introduced gluten at the end of the month. Two people felt better after re-introducing gluten.
Just under half of participants experienced moderate or significant negative symptoms when they re-introduced gluten at the end of the month. Two people felt better after re-introducing gluten.
Conclusion
I find these results striking. Participants overwhelmingly improved in every health category we measured. Although the data may have been somewhat biased due to the 53% response rate, it's indisputable that a large number of participants, probably the majority, benefited from avoiding gluten for a month. At some point, we're going to compile some of the comments people left in the survey, which were overwhelmingly positive. Here's a typical comment in response to the question " In your own words, how would you describe your January 2011 experience" (used with permission):
To get the data I'll be presenting below, first I excluded participants who stated on the survey that they did not adhere to the diet. Next, I excluded participants who were gluten-free before January, because they would presumably not have experienced a change from continuing to avoid gluten. That left us with 53 participants.
For each of these graphs, the vertical axis represents the number of participants in each category. They won't necessarily add up to 53, for several reasons. The most common reason is that for the questions asking about changes in health conditions, I didn't include responses from people who didn't have the condition in question at baseline because there was nothing to change.
Question #1: What is your overall opinion of the effect of gluten free January on you?
 Participants had a very positive experience with the gluten-free diet. Not one person reported a negative overall experience.
Participants had a very positive experience with the gluten-free diet. Not one person reported a negative overall experience.Question #2: Did you note a weight change at the end of gluten free January?
 And here are the data for people who described themselves as overweight at baseline:
And here are the data for people who described themselves as overweight at baseline: Two-thirds of people who were overweight at baseline lost weight, and only one person out of 37 gained weight. That is striking. A number of people didn't weigh themselves, which is why the numbers only add up to 37.
Two-thirds of people who were overweight at baseline lost weight, and only one person out of 37 gained weight. That is striking. A number of people didn't weigh themselves, which is why the numbers only add up to 37.Question #3: Before January 2011, did you have a problem with intestinal transit (frequent constipation or diarrhea)? If so, did your symptoms change during the month of January?
Responses are heavily weighted toward improvement, although there were a few instances where transit worsened. Transit problems are one of the most common manifestations of gluten sensitivity.
Question #4: Before January 2011, did you have frequent digestive discomfort (pain, bloating, etc.)? If so, did your symptoms change during the month of January?

Digestive discomfort was common, and the gluten-free diet improved it in nearly everyone who had it at baseline. I find this really impressive.
Question #5: Before January 2011, did you have acid reflux? If so, did your symptoms change during the month of January?
 Acid reflux responded well to a gluten-free diet.
Acid reflux responded well to a gluten-free diet.Question #6: Before January 2011, did you have a problem with tiredness/lethargy? If so, did your symptoms change during the month of January?
 Lethargy was common and generally improved in people who avoided gluten. This doesn't surprise me at all. The recent controlled gluten study in irritable bowel syndrome patients found that lethargy was the most reliable consequence of eating gluten that they measured (1, 2). That has also been my personal experience.
Lethargy was common and generally improved in people who avoided gluten. This doesn't surprise me at all. The recent controlled gluten study in irritable bowel syndrome patients found that lethargy was the most reliable consequence of eating gluten that they measured (1, 2). That has also been my personal experience.Question #7: Before January 2011, did you have a problem with anxiety? If so, did your symptoms change during the month of January?
 Anxiety tended to improve in most participants who started with it.
Anxiety tended to improve in most participants who started with it.Question #8: Before January 2011, did you have a problem with an autoimmune or inflammatory condition? If so, did your symptoms change during the month of January?
 Autoimmune and inflammatory conditions tended to improve in the gluten-free group, although one person experienced a worsening of symptoms.
Autoimmune and inflammatory conditions tended to improve in the gluten-free group, although one person experienced a worsening of symptoms. Question #9: If you ate gluten again or did a gluten challenge after gluten free January, what was the effect?
 Just under half of participants experienced moderate or significant negative symptoms when they re-introduced gluten at the end of the month. Two people felt better after re-introducing gluten.
Just under half of participants experienced moderate or significant negative symptoms when they re-introduced gluten at the end of the month. Two people felt better after re-introducing gluten.Conclusion
I find these results striking. Participants overwhelmingly improved in every health category we measured. Although the data may have been somewhat biased due to the 53% response rate, it's indisputable that a large number of participants, probably the majority, benefited from avoiding gluten for a month. At some point, we're going to compile some of the comments people left in the survey, which were overwhelmingly positive. Here's a typical comment in response to the question " In your own words, how would you describe your January 2011 experience" (used with permission):
Amazing! I would recommend the experiment to anyone. I felt completely more alert, and less bloated. When I ate some gluten at the close of the experiment, I felt gross, bloated, and lethargic.I think it's worth mentioning that some participants also eliminated other starches, particularly refined starches. Judging by the comments, the diet was probably lower in carbohydrate for a number of participants. We may try to assess that next year.
Monday, March 7, 2011
Flu Season is Here
I've noticed everyone around me getting sick lately (I seem to have become mostly immune to colds and the flu in the last couple of years), so I took a look at Google Flu Trends. Lo and behold, the United States is currently near peak flu incidence for the 2010-2011 season. Here's a graph from Flu Trends. This year's trend is in dark blue:

Flu Trends also has data for individual US states and a number of other countries.
It's time to tighten up your diet and lifestyle if you want to avoid the flu this year. Personally, I feel that eating well, managing stress effectively, and taking 2,000 IU of vitamin D3 per day in winter have helped me avoid colds and the flu.

Flu Trends also has data for individual US states and a number of other countries.
It's time to tighten up your diet and lifestyle if you want to avoid the flu this year. Personally, I feel that eating well, managing stress effectively, and taking 2,000 IU of vitamin D3 per day in winter have helped me avoid colds and the flu.
Thursday, February 24, 2011
Polyphenols, Hormesis and Disease: Part II
In the last post, I explained that the body treats polyphenols as potentially harmful foreign chemicals, or "xenobiotics". How can we reconcile this with the growing evidence that at least a subset of polyphenols have health benefits?
Clues from Ionizing Radiation
One of the more curious things that has been reported in the scientific literature is that although high-dose ionizing radiation (such as X-rays) is clearly harmful, leading to cancer, premature aging and other problems, under some conditions low-dose ionizing radiation can actually decrease cancer risk and increase resistance to other stressors (1, 2, 3, 4, 5). It does so by triggering a protective cellular response, increasing cellular defenses out of proportion to the minor threat posed by the radiation itself. The ability of mild stressors to increase stress resistance is called "hormesis." Exercise is a common example. I've written about this phenomenon in the past (6).
The Case of Resveratrol
Resveratrol is perhaps the most widely known polyphenol, available in supplement stores nationwide. It's seen a lot of hype, being hailed as a "calorie restriction mimetic" and the reason for the "French paradox."* But there is quite a large body of evidence suggesting that resveratrol functions in the same manner as low-dose ionizing radiation and other bioactive polyphenols: by acting as a mild toxin that triggers a hormetic response (7). Just as in the case of radiation, high doses of resveratrol are harmful rather than helpful. This has obvious implications for the supplementation of resveratrol and other polyphenols. A recent review article on polyphenols stated that while dietary polyphenols may be protective, "high-dose fortified foods or dietary supplements are of unproven efficacy and possibly harmful" (8).
The Cellular Response to Oxidants
Although it may not be obvious, radiation and polyphenols activate a cellular response that is similar in many ways. Both activate the transcription factor Nrf2, which activates genes that are involved in detoxification of chemicals and antioxidant defense**(9, 10, 11, 12). This is thought to be due to the fact that polyphenols, just like radiation, may temporarily increase the level of oxidative stress inside cells. Here's a quote from the polyphenol review article quoted above (13):
Nrf2 is one of the main pathways by which polyphenols increase stress resistance and antioxidant defenses, including the key cellular antioxidant glutathione (14). Nrf2 activity is correlated with longevity across species (15). Inducing Nrf2 activity via polyphenols or by other means substantially reduces the risk of common lifestyle disorders in animal models, including cardiovascular disease, diabetes and cancer (16, 17, 18), although Nrf2 isn't necessarily the only mechanism. The human evidence is broadly consistent with the studies in animals, although not as well developed.
One of the most interesting effects of hormesis is that exposure to one stressor can increase resistance to other stressors. For example, long-term consumption of high-polyphenol chocolate increases sunburn resistance in humans, implying that it induces a hormetic response in skin (19). Polyphenol-rich foods such as green tea reduce sunburn and skin cancer development in animals (20, 21).
Chris Masterjohn first introduced me to Nrf2 and the idea that polyphenols act through hormesis. Chris studies the effects of green tea on health, which seem to be mediated by polyphenols.
A Second Mechanism
There is a place in the body where polyphenols are concentrated enough to be direct antioxidants: in the digestive tract after consuming polyphenol-rich foods. Digestion is a chemically harsh process that readily oxidizes ingested substances such as polyunsaturated fats (22). Oxidized fat is neither healthy when it's formed in the deep fryer, nor when it's formed in the digestive tract (23, 24). Eating polyphenol-rich foods effectively prevents these fats from being oxidized during digestion (25). One consequence of this appears to be better absorption and assimilation of the exceptionally fragile omega-3 polyunsaturated fatty acids (26).
What does it all Mean?
I think that overall, the evidence suggests that polyphenol-rich foods are healthy in moderation, and eating them on a regular basis is generally a good idea. Certain other plant chemicals, such as suforaphane found in cruciferous vegetables, and allicin found in garlic, exhibit similar effects and may also act by hormesis (27). Some of the best-studied polyphenol-rich foods are tea (particularly green tea), blueberries, extra-virgin olive oil, red wine, citrus fruits, hibiscus tea, soy, dark chocolate, coffee, turmeric and other herbs and spices, and a number of traditional medicinal herbs. A good rule of thumb is to "eat the rainbow", choosing foods with a variety of colors.
Supplementing with polyphenols and other plant chemicals in amounts that would not be achievable by eating food is probably not a good idea.
* The "paradox" whereby the French eat a diet rich in saturated fat, yet have a low heart attack risk compared to other affluent Western nations.
** Genes containing an antioxidant response element (ARE) in the promoter region. ARE is also sometimes called the electrophile response element (EpRE).
Clues from Ionizing Radiation
One of the more curious things that has been reported in the scientific literature is that although high-dose ionizing radiation (such as X-rays) is clearly harmful, leading to cancer, premature aging and other problems, under some conditions low-dose ionizing radiation can actually decrease cancer risk and increase resistance to other stressors (1, 2, 3, 4, 5). It does so by triggering a protective cellular response, increasing cellular defenses out of proportion to the minor threat posed by the radiation itself. The ability of mild stressors to increase stress resistance is called "hormesis." Exercise is a common example. I've written about this phenomenon in the past (6).
The Case of Resveratrol
Resveratrol is perhaps the most widely known polyphenol, available in supplement stores nationwide. It's seen a lot of hype, being hailed as a "calorie restriction mimetic" and the reason for the "French paradox."* But there is quite a large body of evidence suggesting that resveratrol functions in the same manner as low-dose ionizing radiation and other bioactive polyphenols: by acting as a mild toxin that triggers a hormetic response (7). Just as in the case of radiation, high doses of resveratrol are harmful rather than helpful. This has obvious implications for the supplementation of resveratrol and other polyphenols. A recent review article on polyphenols stated that while dietary polyphenols may be protective, "high-dose fortified foods or dietary supplements are of unproven efficacy and possibly harmful" (8).
The Cellular Response to Oxidants
Although it may not be obvious, radiation and polyphenols activate a cellular response that is similar in many ways. Both activate the transcription factor Nrf2, which activates genes that are involved in detoxification of chemicals and antioxidant defense**(9, 10, 11, 12). This is thought to be due to the fact that polyphenols, just like radiation, may temporarily increase the level of oxidative stress inside cells. Here's a quote from the polyphenol review article quoted above (13):
We have found that [polyphenols] are potentially far more than 'just antioxidants', but that they are probably insignificant players as 'conventional' antioxidants. They appear, under most circumstances, to be just the opposite, i.e. prooxidants, that nevertheless appear to contribute strongly to protection from oxidative stress by inducing cellular endogenous enzymic protective mechanisms. They appear to be able to regulate not only antioxidant gene transcription but also numerous aspects of intracellular signaling cascades involved in the regulation of cell growth, inflammation and many other processes.It's worth noting that this is essentially the opposite of what you'll hear on the evening news, that polyphenols are direct antioxidants. The scientific cutting edge has largely discarded that hypothesis, but the mainstream has not yet caught on.
Nrf2 is one of the main pathways by which polyphenols increase stress resistance and antioxidant defenses, including the key cellular antioxidant glutathione (14). Nrf2 activity is correlated with longevity across species (15). Inducing Nrf2 activity via polyphenols or by other means substantially reduces the risk of common lifestyle disorders in animal models, including cardiovascular disease, diabetes and cancer (16, 17, 18), although Nrf2 isn't necessarily the only mechanism. The human evidence is broadly consistent with the studies in animals, although not as well developed.
One of the most interesting effects of hormesis is that exposure to one stressor can increase resistance to other stressors. For example, long-term consumption of high-polyphenol chocolate increases sunburn resistance in humans, implying that it induces a hormetic response in skin (19). Polyphenol-rich foods such as green tea reduce sunburn and skin cancer development in animals (20, 21).
Chris Masterjohn first introduced me to Nrf2 and the idea that polyphenols act through hormesis. Chris studies the effects of green tea on health, which seem to be mediated by polyphenols.
A Second Mechanism
There is a place in the body where polyphenols are concentrated enough to be direct antioxidants: in the digestive tract after consuming polyphenol-rich foods. Digestion is a chemically harsh process that readily oxidizes ingested substances such as polyunsaturated fats (22). Oxidized fat is neither healthy when it's formed in the deep fryer, nor when it's formed in the digestive tract (23, 24). Eating polyphenol-rich foods effectively prevents these fats from being oxidized during digestion (25). One consequence of this appears to be better absorption and assimilation of the exceptionally fragile omega-3 polyunsaturated fatty acids (26).
What does it all Mean?
I think that overall, the evidence suggests that polyphenol-rich foods are healthy in moderation, and eating them on a regular basis is generally a good idea. Certain other plant chemicals, such as suforaphane found in cruciferous vegetables, and allicin found in garlic, exhibit similar effects and may also act by hormesis (27). Some of the best-studied polyphenol-rich foods are tea (particularly green tea), blueberries, extra-virgin olive oil, red wine, citrus fruits, hibiscus tea, soy, dark chocolate, coffee, turmeric and other herbs and spices, and a number of traditional medicinal herbs. A good rule of thumb is to "eat the rainbow", choosing foods with a variety of colors.
Supplementing with polyphenols and other plant chemicals in amounts that would not be achievable by eating food is probably not a good idea.
* The "paradox" whereby the French eat a diet rich in saturated fat, yet have a low heart attack risk compared to other affluent Western nations.
** Genes containing an antioxidant response element (ARE) in the promoter region. ARE is also sometimes called the electrophile response element (EpRE).
Thursday, January 27, 2011
The Diabetes Epidemic
The CDC just released its latest estimate of diabetes prevalence in the US (1):
These data are self-reported, and do not correct for differences in diagnosis methods, so they should be viewed with caution-- but they still serve to illustrate the trend. There was an increase in diabetes incidence that began in the early 1990s. More than 90 percent of cases are type 2 diabetics. Disturbingly, the trend does not show any signs of slowing.
The diabetes epidemic has followed on the heels of the obesity epidemic with 10-20 years of lag time. Excess body fat is the number one risk factor for diabetes*. As far as I can tell, type 2 diabetes is caused by insulin resistance, which is probably due to energy intake exceeding energy needs (overnutrition), causing a state of cellular insulin resistance as a defense mechanism to protect against the damaging effects of too much glucose and fatty acids (3). In addition, type 2 diabetes requires a predisposition that prevents the pancreatic beta cells from keeping up with the greatly increased insulin needs of an insulin resistant person**. Both factors are required, and not all insulin resistant people will develop diabetes as some people's beta cells are able to compensate by hypersecreting insulin.
Why does energy intake exceed energy needs in modern America and in most affluent countries? Why has the typical person's calorie intake increased by 250 calories per day since 1970 (4)? I believe it's because the fat mass "setpoint" has been increased, typically but not always by industrial food. I've been developing some new thoughts on this lately, and potentially new solutions, which I'll reveal when they're ready.
* In other words, it's the best predictor of future diabetes risk.
** Most of the common gene variants (of known function) linked with type 2 diabetes are thought to impact beta cell function (5).
Diabetes affects 8.3 percent of Americans of all ages, and 11.3 percent of adults aged 20 and older, according to the National Diabetes Fact Sheet for 2011. About 27 percent of those with diabetes�7 million Americans�do not know they have the disease. Prediabetes affects 35 percent of adults aged 20 and older.Wow-- this is a massive problem. The prevalence of diabetes has been increasing over time, due to more people developing the disorder, improvements in diabetes care leading to longer survival time, and changes in the way diabetes is diagnosed. Here's a graph I put together based on CDC data, showing the trend of diabetes prevalence (percent) from 1980 to 2008 in different age categories (2):
These data are self-reported, and do not correct for differences in diagnosis methods, so they should be viewed with caution-- but they still serve to illustrate the trend. There was an increase in diabetes incidence that began in the early 1990s. More than 90 percent of cases are type 2 diabetics. Disturbingly, the trend does not show any signs of slowing.

{kind=link}
The diabetes epidemic has followed on the heels of the obesity epidemic with 10-20 years of lag time. Excess body fat is the number one risk factor for diabetes*. As far as I can tell, type 2 diabetes is caused by insulin resistance, which is probably due to energy intake exceeding energy needs (overnutrition), causing a state of cellular insulin resistance as a defense mechanism to protect against the damaging effects of too much glucose and fatty acids (3). In addition, type 2 diabetes requires a predisposition that prevents the pancreatic beta cells from keeping up with the greatly increased insulin needs of an insulin resistant person**. Both factors are required, and not all insulin resistant people will develop diabetes as some people's beta cells are able to compensate by hypersecreting insulin.
Why does energy intake exceed energy needs in modern America and in most affluent countries? Why has the typical person's calorie intake increased by 250 calories per day since 1970 (4)? I believe it's because the fat mass "setpoint" has been increased, typically but not always by industrial food. I've been developing some new thoughts on this lately, and potentially new solutions, which I'll reveal when they're ready.
* In other words, it's the best predictor of future diabetes risk.
** Most of the common gene variants (of known function) linked with type 2 diabetes are thought to impact beta cell function (5).
Thursday, January 20, 2011
Eating Wheat Gluten Causes Symptoms in Some People Who Don't Have Celiac Disease
Irritable bowel syndrome (IBS) is a condition characterized by the frequent occurrence of abdominal pain, diarrhea, constipation, bloating and/or gas. If that sounds like an extremely broad description, that's because it is. The word "syndrome" is medicalese for "we don't know what causes it." IBS seems to be a catch-all for various persistent digestive problems that aren't defined as separate disorders, and it has a very high prevalence: as high as 14 percent of people in the US, although the estimates depend on what diagnostic criteria are used (1). It can be brought on or exacerbated by several different types of stressors, including emotional stress and infection.
Mael�n Fontes Villalba at Lund University recently forwarded me an interesting new paper in the American Journal of Gastroenterology (2). Dr. Jessica R. Biesiekierski and colleagues recruited 34 IBS patients who did not have celiac disease, but who felt they had benefited from going gluten-free in their daily lives*. All patients continued on their pre-study gluten-free diet, however, all participants were provided with two slices of gluten-free bread and one gluten-free muffin per day. The investigators added isolated wheat gluten to the bread and muffins of half the study group.
During the six weeks of the intervention, patients receiving the gluten-free food fared considerably better on nearly every symptom of IBS measured. The most striking difference was in tiredness-- the gluten-free group was much less tired on average than the gluten group. Interestingly, they found that a negative reaction to gluten was not necessarily accompanied by the presence of anti-gluten antibodies in the blood, which is a test often used to diagnose gluten sensitivity.
Here's what I take away from this study:
I don't expect everyone to benefit from avoiding gluten. But for those who are really sensitive, it can make a huge difference. Digestive, autoimmune and neurological disorders associate most strongly with gluten sensitivity. Avoiding gluten can be a fruitful thing to try in cases of mysterious chronic illness. We're two-thirds of the way through Gluten-Free January. I've been fastidiously avoiding gluten, as annoying as it's been at times***. Has anyone noticed a change in their health?
* 56% of volunteers carried HLA-DQ2 or DQ8 alleles, which is slightly higher than the general population. Nearly all people with celiac disease carry one of these two alleles. 28% of volunteers were positive for anti-gliadin IgA, which is higher than the general population.
** Some people feel they are reacting to the fructans in wheat, rather than the gluten. If a modest amount of onion causes the same symptoms as eating wheat, then that may be true. If not, then it's probably the gluten.
*** I'm usually about 95% gluten-free anyway. But when I want a real beer, I want one brewed with barley. And when I want Thai food or sushi, I don't worry about a little bit of wheat in the soy sauce. If a friend makes me food with gluten in it, I'll eat it and enjoy it. This month I'm 100% gluten-free though, because I can't in good conscience encourage my blog readership to try it if I'm not doing it myself. At the end of the month, I'm going to do a blinded gluten challenge (with a gluten-free control challenge) to see once and for all if I react to it. Stay tuned for more on that.
Mael�n Fontes Villalba at Lund University recently forwarded me an interesting new paper in the American Journal of Gastroenterology (2). Dr. Jessica R. Biesiekierski and colleagues recruited 34 IBS patients who did not have celiac disease, but who felt they had benefited from going gluten-free in their daily lives*. All patients continued on their pre-study gluten-free diet, however, all participants were provided with two slices of gluten-free bread and one gluten-free muffin per day. The investigators added isolated wheat gluten to the bread and muffins of half the study group.
During the six weeks of the intervention, patients receiving the gluten-free food fared considerably better on nearly every symptom of IBS measured. The most striking difference was in tiredness-- the gluten-free group was much less tired on average than the gluten group. Interestingly, they found that a negative reaction to gluten was not necessarily accompanied by the presence of anti-gluten antibodies in the blood, which is a test often used to diagnose gluten sensitivity.
Here's what I take away from this study:
- Wheat gluten can cause symptoms in susceptible people who do not have celiac disease.
- A lack of circulating antibodies against gluten does not necessarily indicate a lack of gluten sensitivity.
- People with mysterious digestive problems may want to try avoiding gluten for a while to see if it improves their symptoms**.
- People with mysterious fatigue may want to try avoiding gluten.
I don't expect everyone to benefit from avoiding gluten. But for those who are really sensitive, it can make a huge difference. Digestive, autoimmune and neurological disorders associate most strongly with gluten sensitivity. Avoiding gluten can be a fruitful thing to try in cases of mysterious chronic illness. We're two-thirds of the way through Gluten-Free January. I've been fastidiously avoiding gluten, as annoying as it's been at times***. Has anyone noticed a change in their health?
* 56% of volunteers carried HLA-DQ2 or DQ8 alleles, which is slightly higher than the general population. Nearly all people with celiac disease carry one of these two alleles. 28% of volunteers were positive for anti-gliadin IgA, which is higher than the general population.
** Some people feel they are reacting to the fructans in wheat, rather than the gluten. If a modest amount of onion causes the same symptoms as eating wheat, then that may be true. If not, then it's probably the gluten.
*** I'm usually about 95% gluten-free anyway. But when I want a real beer, I want one brewed with barley. And when I want Thai food or sushi, I don't worry about a little bit of wheat in the soy sauce. If a friend makes me food with gluten in it, I'll eat it and enjoy it. This month I'm 100% gluten-free though, because I can't in good conscience encourage my blog readership to try it if I'm not doing it myself. At the end of the month, I'm going to do a blinded gluten challenge (with a gluten-free control challenge) to see once and for all if I react to it. Stay tuned for more on that.
Thursday, August 12, 2010
Can a Statin Neutralize the Cardiovascular Risk of Unhealthy Dietary Choices?
The title of this post is the exact title of a recent editorial in the American Journal of Cardiology (1). Investigators calculated the "risk for cardiovascular disease associated with the total fat and trans fat content of fast foods", and compared it to the "risk decrease provided by daily statin consumption". Here's what they found:
I can't be sure, but I think there's a pretty good chance the authors were being facetious in this editorial, in which case I think a) it's hilarious, b) most people aren't going to get the joke. If they are joking, the editorial is designed to shine a light on the sad state of mainstream preventive healthcare. Rather than trying to educate people and change the deadly industrial food system, which is at the root of a constellation of health problems, many people think it's acceptable to partially correct one health risk by tinkering with the human metabolism using drugs. To be fair, most people aren't willing to change their diet and lifestyle habits (and perhaps for some it's even too late), so frustrated physicians prescribe drugs to mitigate the risk. I accept that. But if our society is really committed to its own health and well-being, we'll remove the artificial incentives that favor industrial food, and educate children from a young age on how to eat well.
I think one of the main challenges we face is that our current system is immensely lucrative for powerful financial interests. Industrial agriculture lines the pockets of a few large farmers and executives (while smaller farmers go broke and get bought out), industrial food processing concentrates profit among a handful of mega-manufacturers, and then people who are made ill by the resulting food spend an exorbitant amount of money on increasingly sophisticated (and expensive) healthcare. It's a system that effectively milks US citizens for a huge amount of money, and keeps the economy rolling at the expense of the average person's well-being. All of these groups have powerful lobbies that ensure the continuity of the current system. Litigation isn't the main reason our healthcare is so expensive in the US; high levels of chronic disease, expensive new technology, a "kitchen sink" treatment approach, and inefficient private companies are the real reasons.
If the editorial is serious, there are so many things wrong with it I don't even know where to begin. Here are a few problems:
The risk reduction associated with the daily consumption of most statins, with the exception of pravastatin, is more powerful than the risk increase caused by the daily extra fat intake associated with a 7-oz hamburger (Quarter Pounder�) with cheese and a small milkshake. In conclusion, statin therapy can neutralize the cardiovascular risk caused by harmful diet choices.Wow. Later in the editorial, they recommend "a new and protective packet, �MacStatin,� which could be sprinkled onto a Quarter Pounder or into a milkshake." I'm not making this up!
Routine accessibility of statins in establishments providing unhealthy food might be a rational modern means to offset the cardiovascular risk. Fast food outlets already offer free condiments to supplement meals. A free statin-containing accompaniment would offer cardiovascular benefits, opposite to the effects of equally available salt, sugar, and high-fat condiments. Although no substitute for systematic lifestyle improvements, including healthy diet, regular exercise, weight loss, and smoking cessation, complimentary statin packets would add, at little cost, 1 positive choice to a panoply of negative ones.
I can't be sure, but I think there's a pretty good chance the authors were being facetious in this editorial, in which case I think a) it's hilarious, b) most people aren't going to get the joke. If they are joking, the editorial is designed to shine a light on the sad state of mainstream preventive healthcare. Rather than trying to educate people and change the deadly industrial food system, which is at the root of a constellation of health problems, many people think it's acceptable to partially correct one health risk by tinkering with the human metabolism using drugs. To be fair, most people aren't willing to change their diet and lifestyle habits (and perhaps for some it's even too late), so frustrated physicians prescribe drugs to mitigate the risk. I accept that. But if our society is really committed to its own health and well-being, we'll remove the artificial incentives that favor industrial food, and educate children from a young age on how to eat well.
I think one of the main challenges we face is that our current system is immensely lucrative for powerful financial interests. Industrial agriculture lines the pockets of a few large farmers and executives (while smaller farmers go broke and get bought out), industrial food processing concentrates profit among a handful of mega-manufacturers, and then people who are made ill by the resulting food spend an exorbitant amount of money on increasingly sophisticated (and expensive) healthcare. It's a system that effectively milks US citizens for a huge amount of money, and keeps the economy rolling at the expense of the average person's well-being. All of these groups have powerful lobbies that ensure the continuity of the current system. Litigation isn't the main reason our healthcare is so expensive in the US; high levels of chronic disease, expensive new technology, a "kitchen sink" treatment approach, and inefficient private companies are the real reasons.
If the editorial is serious, there are so many things wrong with it I don't even know where to begin. Here are a few problems:
- They assume the risk of heart attack conveyed by eating fast food is due to its total and trans fat content, which is simplistic. To support that supposition, they cite one study: the Health Professionals Follow-up Study (2). This is one of the best diet-health observational studies conducted to date. The authors of the editorial appear not to have read the study carefully, because it found no association between total or saturated fat intake and heart attack risk, when adjusted for confounding variables. The number they quoted (relative risk = 1.23) was before adjustment for fiber intake (relative risk = 1.02 after adjustment), and in any case, it was not statistically significant even before adjustment. How did that get past peer review? Answer: reviewers aren't critical of hypotheses they like.
- Statins mostly work in middle-aged men, and reduce the risk of heart attack by about one quarter. The authors excluded several recent unsupportive trials from their analysis. Dr. Michel de Lorgeril reviewed these trials recently (3). For these reasons, adding a statin to fast food would probably have a negligible effect on the heart attack risk of the general population.
- "Statins rarely cause negative side effects." BS. Of the half dozen people I know who have gone on statins, all of them have had some kind of negative side effect, two of them unpleasant enough that they discontinued treatment against their doctor's wishes. Several of them who remained on statins are unlikely to benefit because of their demographic, yet they remain on statins on their doctors' advice.
- Industrial food is probably the main contributor to heart attack risk. Cultures that don't eat industrial food are almost totally free of heart attacks, as demonstrated by a variety of high-quality studies (4, 5, 6, 7, 8, 9). No drug can replicate that, not even close.
Thursday, July 8, 2010
China Study Problems of Interpretation
The China study was an observational study that collected a massive amount of information about diet and health in 65 different rural regions of China. It's been popularized by Dr. T. Colin Campbell, who has argued that the study shows that plant foods are generally superior to animal foods for health, and even a small amount of animal food is harmful. Campbell's book has been at the center of the strict vegetarian (vegan) movement since its publication.
Richard from Free the Animal just passed on some information that many of you may find interesting. A woman named Denise Minger recently published a series of posts on the China study. She looked up the raw data and applied statistics to it. It's the most thorough review of the data I've seen so far. She raises some points about Campbell's interpretation of the data that are frankly disturbing. As I like to say, the problem is usually not in the data-- it's in the interpretation.
One of the things Minger points out is that wheat intake had a massive correlation with coronary heart disease-- one of the strongest correlations the investigators found. Is that because wheat causes CHD, or is it because wheat eating regions tend to be further North and thus have worse vitamin D status? I don't know, but it's an interesting observation nevertheless. Check out Denise Minger's posts... if you have the stamina:
The China Study: Fact or Fallacy
Also, see posts on the China study by Richard Nikoley, Chris Masterjohn and Anthony Colpo:
T. Colin Campbell's the China Study
The Truth About the China Study
The China Study: More Vegan Nonsense
And my previous post on the association between wheat intake and obesity in China:
Wheat in China
Richard from Free the Animal just passed on some information that many of you may find interesting. A woman named Denise Minger recently published a series of posts on the China study. She looked up the raw data and applied statistics to it. It's the most thorough review of the data I've seen so far. She raises some points about Campbell's interpretation of the data that are frankly disturbing. As I like to say, the problem is usually not in the data-- it's in the interpretation.
One of the things Minger points out is that wheat intake had a massive correlation with coronary heart disease-- one of the strongest correlations the investigators found. Is that because wheat causes CHD, or is it because wheat eating regions tend to be further North and thus have worse vitamin D status? I don't know, but it's an interesting observation nevertheless. Check out Denise Minger's posts... if you have the stamina:
The China Study: Fact or Fallacy
Also, see posts on the China study by Richard Nikoley, Chris Masterjohn and Anthony Colpo:
T. Colin Campbell's the China Study
The Truth About the China Study
The China Study: More Vegan Nonsense
And my previous post on the association between wheat intake and obesity in China:
Wheat in China
Saturday, July 3, 2010
Tropical Plant Fats: Palm Oil
A Fatal Case of Nutritionism
The concept of 'nutritionism' was developed by Dr. Gyorgy Scrinis and popularized by the food writer Michael Pollan. It states that the health value of a food can be guessed by the sum of the nutrients it contains. Pollan argues, I think rightfully, that nutritionism is a reductionist philosophy that assumes we know more about food composition and the human body than we actually do. You can find varying degrees of this philosophy in most mainstream discussions of diet and health*.
One conspicuous way nutritionism manifests is in the idea that saturated fat is harmful. Any fat rich in saturated fatty acids is typically assumed to be unhealthy, regardless of its other constituents. There is also apparently no need to directly test that assumption, or even to look through the literature to see if the assumption has already been tested. In this manner, 'saturated' tropical plant fats such as palm oil and coconut oil have been labeled unhealthy, despite essentially no direct evidence that they're harmful. As we'll see, there is actually quite a bit of evidence, both indirect and direct, that their unrefined forms are not harmful and perhaps even beneficial.
Palm Oil and Heart Disease
Long-time readers may recall a post I wrote a while back titled Ischemic Heart Attacks: Disease of Civilization (1). I described a study from 1964 in which investigators looked for signs of heart attacks in thousands of consecutive autopsies in the US and Africa, among other places. They found virtually none in hearts from Nigeria and Uganda (3 non-fatal among more than 4,500 hearts), while Americans of the same age had very high rates (up to 1/3 of hearts).
What do they eat in Nigeria? Typical Nigerian food involves home-processed grains, starchy root vegetables, beans, fruit, vegetables, peanuts, red palm oil, and a bit of dairy, fish and meat**. The oil palm Elaeis guineensis originated in West Africa and remains one of the main dietary fats throughout the region.
To extract the oil, palm fruit are steamed, and the oily flesh is removed and pressed. It's similar to olive oil in that it is extracted gently from an oil-rich fruit, rather than harshly from an oil-poor seed (e.g., corn or soy oil). The oil that results is deep red and is perhaps the most nutrient-rich fat on the planet. The red color comes from carotenes, but red palm oil also contains a large amount of vitamin E (mostly tocotrienols), vitamin K1, coenzyme Q10 and assorted other fat-soluble constituents. This adds up to a very high concentration of fat-soluble antioxidants, which are needed to protect the fat from rancidity in hot and sunny West Africa. Some of these make it into the body when it's ingested, where they appear to protect the body's own fats from oxidation.
Mainstream nutrition authorities state that palm oil should be avoided due to the fact that it's approximately half saturated. This is actually one of the main reasons palm oil was replaced by hydrogenated seed oils in the processed food industry. Saturated fat raises blood cholesterol, which increases the risk of heart disease. Doesn't it? Let's see what the studies have to say.
Most of the studies were done using refined palm oil, unfortunately. Besides only being relevant to processed foods, this method also introduces a new variable because palm oil can be refined and oxidized to varying degrees. However, a few studies were done with red palm oil, and one even compared it to refined palm oil. Dr. Suzanna Scholtz and colleagues put 59 volunteers on diets predominating in sunflower oil, refined palm oil or red palm oil for 4 weeks. LDL cholesterol was not different between the sunflower oil and red palm oil groups, however the red palm oil group saw a significant increase in HDL. LDL and HDL both increased in the refined palm oil group relative to the sunflower oil group (2).
Although the evidence is conflicting, most studies have not been able to replicate the finding that refined palm oil increases LDL relative to less saturated oils (3, 4). This is consistent with studies in a variety of species showing that saturated fat generally doesn't raise LDL compared to monounsaturated fat in the long term, unless a large amount of purified cholesterol is added to the diet (5).
Investigators have also explored the ability of palm oil to promote atherosclerosis, or hardening and thickening of the arteries, in animals. Not only does palm oil not promote atherosclerosis relative to monounsaturated fats (e.g., olive oil), but in its unrefined state it actually protects against atherosclerosis (6, 7). A study in humans hinted at a possible explanation: compared to a monounsaturated oil***, palm oil greatly reduced oxidized LDL (8). As a matter of fact, I've never seen a dietary intervention reduce oxLDL to that degree (69%). oxLDL is a major risk factor for cardiovascular disease, and a much better predictor of risk than the typically measured LDL cholesterol (9). The paper didn't state whether or not the palm oil was refined. I suspect it was lightly refined, but still rich in vitamin E and CoQ10.
As I discussed in my recent interview with Jimmy Moore, atherosclerosis is only one factor in heart attack risk (10). Several other factors are also major determinants of risk: clotting tendency, plaque stability, and susceptibility to arrhythmia. Another factor that I haven't discussed is how resistant the heart muscle is to hypoxia, or loss of oxygen. If the coronary arteries are temporarily blocked-- a frequent occurrence in modern people-- the heart muscle can be damaged. Dietary factors determine the degree of damage that results. For example, in rodents, nitrites derived from green vegetables protect the heart from hypoxia damage (11). It turns out that red palm oil is also protective (12, 13). Red palm oil also protects against high blood pressure in rats, an effect attributed to its ability to reduce oxidative stress (14, 15).
Together, the evidence suggests that red palm oil does not contribute to heart disease risk, and in fact is likely to be protective. The benefits of red palm oil probably come mostly from its minor constituents, i.e. the substances besides its fatty acids. Several studies have shown that a red palm oil extract called palmvitee lowers serum lipids in humans (16, 17). The minor constituents are precisely what are removed during the refining process.
Palm Oil and the Immune System
Red palm oil also has beneficial effects on the immune system in rodents. It protects against bacterial infection when compared with soybean oil (18). It also protects against certain cancers, compared to other oils (19, 20). This may be in part due to its lower content of omega-6 linoleic acid (roughly 10%), and minor constituents.
The Verdict
Yet again, nutritionism has gotten itself into trouble by underestimating the biological complexity of a whole food. Rather than being harmful to human health, red palm oil, an ancient and delicious food, is likely to be protective. It's also one of the cheapest oils available worldwide, due to the oil palm's high productivity. It has a good shelf life and does not require refrigeration. Its strong, savory flavor goes well in stews, particularly meat stews. It isn't available in most grocery stores, but you can find it on the internet. Make sure not to confuse it with refined palm oil or palm kernel oil.
* The approach that Pollan and I favor is a simpler, more empirical one: eat foods that have successfully sustained healthy cultures.
** Some Nigerians are also pastoralists that subsist primarily on dairy.
*** High oleic sunflower oil, from a type of sunflower bred to be high in monounsaturated fat and low in linoleic acid. I think it's probably among the least harmful refined oils. I use it sometimes to make mayonnaise. It's often available in grocery stores, just check the label.
The concept of 'nutritionism' was developed by Dr. Gyorgy Scrinis and popularized by the food writer Michael Pollan. It states that the health value of a food can be guessed by the sum of the nutrients it contains. Pollan argues, I think rightfully, that nutritionism is a reductionist philosophy that assumes we know more about food composition and the human body than we actually do. You can find varying degrees of this philosophy in most mainstream discussions of diet and health*.
One conspicuous way nutritionism manifests is in the idea that saturated fat is harmful. Any fat rich in saturated fatty acids is typically assumed to be unhealthy, regardless of its other constituents. There is also apparently no need to directly test that assumption, or even to look through the literature to see if the assumption has already been tested. In this manner, 'saturated' tropical plant fats such as palm oil and coconut oil have been labeled unhealthy, despite essentially no direct evidence that they're harmful. As we'll see, there is actually quite a bit of evidence, both indirect and direct, that their unrefined forms are not harmful and perhaps even beneficial.
Palm Oil and Heart Disease
Long-time readers may recall a post I wrote a while back titled Ischemic Heart Attacks: Disease of Civilization (1). I described a study from 1964 in which investigators looked for signs of heart attacks in thousands of consecutive autopsies in the US and Africa, among other places. They found virtually none in hearts from Nigeria and Uganda (3 non-fatal among more than 4,500 hearts), while Americans of the same age had very high rates (up to 1/3 of hearts).
What do they eat in Nigeria? Typical Nigerian food involves home-processed grains, starchy root vegetables, beans, fruit, vegetables, peanuts, red palm oil, and a bit of dairy, fish and meat**. The oil palm Elaeis guineensis originated in West Africa and remains one of the main dietary fats throughout the region.
To extract the oil, palm fruit are steamed, and the oily flesh is removed and pressed. It's similar to olive oil in that it is extracted gently from an oil-rich fruit, rather than harshly from an oil-poor seed (e.g., corn or soy oil). The oil that results is deep red and is perhaps the most nutrient-rich fat on the planet. The red color comes from carotenes, but red palm oil also contains a large amount of vitamin E (mostly tocotrienols), vitamin K1, coenzyme Q10 and assorted other fat-soluble constituents. This adds up to a very high concentration of fat-soluble antioxidants, which are needed to protect the fat from rancidity in hot and sunny West Africa. Some of these make it into the body when it's ingested, where they appear to protect the body's own fats from oxidation.
Mainstream nutrition authorities state that palm oil should be avoided due to the fact that it's approximately half saturated. This is actually one of the main reasons palm oil was replaced by hydrogenated seed oils in the processed food industry. Saturated fat raises blood cholesterol, which increases the risk of heart disease. Doesn't it? Let's see what the studies have to say.
Most of the studies were done using refined palm oil, unfortunately. Besides only being relevant to processed foods, this method also introduces a new variable because palm oil can be refined and oxidized to varying degrees. However, a few studies were done with red palm oil, and one even compared it to refined palm oil. Dr. Suzanna Scholtz and colleagues put 59 volunteers on diets predominating in sunflower oil, refined palm oil or red palm oil for 4 weeks. LDL cholesterol was not different between the sunflower oil and red palm oil groups, however the red palm oil group saw a significant increase in HDL. LDL and HDL both increased in the refined palm oil group relative to the sunflower oil group (2).
Although the evidence is conflicting, most studies have not been able to replicate the finding that refined palm oil increases LDL relative to less saturated oils (3, 4). This is consistent with studies in a variety of species showing that saturated fat generally doesn't raise LDL compared to monounsaturated fat in the long term, unless a large amount of purified cholesterol is added to the diet (5).
Investigators have also explored the ability of palm oil to promote atherosclerosis, or hardening and thickening of the arteries, in animals. Not only does palm oil not promote atherosclerosis relative to monounsaturated fats (e.g., olive oil), but in its unrefined state it actually protects against atherosclerosis (6, 7). A study in humans hinted at a possible explanation: compared to a monounsaturated oil***, palm oil greatly reduced oxidized LDL (8). As a matter of fact, I've never seen a dietary intervention reduce oxLDL to that degree (69%). oxLDL is a major risk factor for cardiovascular disease, and a much better predictor of risk than the typically measured LDL cholesterol (9). The paper didn't state whether or not the palm oil was refined. I suspect it was lightly refined, but still rich in vitamin E and CoQ10.
As I discussed in my recent interview with Jimmy Moore, atherosclerosis is only one factor in heart attack risk (10). Several other factors are also major determinants of risk: clotting tendency, plaque stability, and susceptibility to arrhythmia. Another factor that I haven't discussed is how resistant the heart muscle is to hypoxia, or loss of oxygen. If the coronary arteries are temporarily blocked-- a frequent occurrence in modern people-- the heart muscle can be damaged. Dietary factors determine the degree of damage that results. For example, in rodents, nitrites derived from green vegetables protect the heart from hypoxia damage (11). It turns out that red palm oil is also protective (12, 13). Red palm oil also protects against high blood pressure in rats, an effect attributed to its ability to reduce oxidative stress (14, 15).
Together, the evidence suggests that red palm oil does not contribute to heart disease risk, and in fact is likely to be protective. The benefits of red palm oil probably come mostly from its minor constituents, i.e. the substances besides its fatty acids. Several studies have shown that a red palm oil extract called palmvitee lowers serum lipids in humans (16, 17). The minor constituents are precisely what are removed during the refining process.
Palm Oil and the Immune System
Red palm oil also has beneficial effects on the immune system in rodents. It protects against bacterial infection when compared with soybean oil (18). It also protects against certain cancers, compared to other oils (19, 20). This may be in part due to its lower content of omega-6 linoleic acid (roughly 10%), and minor constituents.
The Verdict
Yet again, nutritionism has gotten itself into trouble by underestimating the biological complexity of a whole food. Rather than being harmful to human health, red palm oil, an ancient and delicious food, is likely to be protective. It's also one of the cheapest oils available worldwide, due to the oil palm's high productivity. It has a good shelf life and does not require refrigeration. Its strong, savory flavor goes well in stews, particularly meat stews. It isn't available in most grocery stores, but you can find it on the internet. Make sure not to confuse it with refined palm oil or palm kernel oil.
* The approach that Pollan and I favor is a simpler, more empirical one: eat foods that have successfully sustained healthy cultures.
** Some Nigerians are also pastoralists that subsist primarily on dairy.
*** High oleic sunflower oil, from a type of sunflower bred to be high in monounsaturated fat and low in linoleic acid. I think it's probably among the least harmful refined oils. I use it sometimes to make mayonnaise. It's often available in grocery stores, just check the label.
Thursday, June 24, 2010
Interview with Jimmy Moore
About two months ago, I did an interview with Jimmy Moore of the Livin' la Vida Low Carb internet empire. I hardly remember what we talked about, but I think it went well. I enjoyed Jimmy's pleasant and open-minded attitude. Head over to Jimmy's website and listen to the interview here.
I do recall making at least one mistake. When discussing heart attacks,I said "atrial fibrillation" when I meant "ventricular fibrillation".
I do recall making at least one mistake. When discussing heart attacks,I said "atrial fibrillation" when I meant "ventricular fibrillation".
Subscribe to:
Posts (Atom)